Abstract
Introduction: Vallecular cyst is a mucous retention cyst that forms between the base of the tongue and the lingual surface of the epiglottis. Our objective was the diagnostic, therapeutic and progressive aspects. Case report: This was a 6-year-old female patient, a student, residing in Kayes with no medical or surgical history, who was admitted for progressive pharyngeal discomfort that had been developing for 3 months. At the nasofibroscopy we highlighted a soft, oval, transluminal mass, with regular contours, non-painful, non-bleeding on contact, measuring approximately 5 cm in diameter at the level of the right vallecula. The rest of the examination of the other devices was normal. We concluded that it was a vallecula cyst. A coordinated airway management plan was established by the anesthesiologist-surgeon before the procedure. Excisional surgery was performed under general anesthesia with orotracheal intubation. The histological result of the surgical specimen concluded that there was fibrous and inflammatory squamous tissue. After six months of follow-up, we have not noted any recurrence. Conclusion: Vallecular cyst is a rare and potentially fatal condition in children due to narrowness of the laryngeal passage. vallecular cyst can be discovered at any age. Laryngeal endoscopy allows diagnosis to be made and treatment is surgical either by endoscopic route or by external cervical route
1. Introduction
Vallecular cyst is a mucous retention cyst that forms between the base of the tongue and the lingual surface of the epiglottis
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
[1]
. It is a rare benign lesion developed at the expense of mucous glands of the vallecular
. It is a rare cause in children, they represent 10.5 to 20.1% of all laryngeal cysts
| [3] | Lengane NI, Ouermi AS, Some MJ, Coulibaly A, Kadyogo M, et al. Vallecular cyst in children: a report of 3 cases. African Journal of Clinical Cases and Reviews 2020; 4(3): 287-90. |
[3]
. Symptoms can be found at any age but can be critical in neonates. The diagnosis is based on clinical examination but especially on endoscopy which will determine the subsequent management
| [4] | Hariga I, Mardassi A, Zribi S, Charfeddine A, Amor MB, Gamra OB, et al. The vallecula cyst: about 2 observations. J. TUN ORL 2008; 20: 45-48. |
[4]
. The severity of the symptoms is variable, most often caused by laryngeal dyspnea characterized by stridor, inspiratory bradypnea, intercostal indrawing and apneas
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
| [3] | Lengane NI, Ouermi AS, Some MJ, Coulibaly A, Kadyogo M, et al. Vallecular cyst in children: a report of 3 cases. African Journal of Clinical Cases and Reviews 2020; 4(3): 287-90. |
[1, 3]
. Dysphagia is rarely the major symptom in children
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
[1]
. It is responsible for airway obstruction that can be life-threatening
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
[1]
. La nasofibroscopie permet de diagnostiquer le kyste, bien que le diagnostic peut passer in apercu si attention n’est pas portée sur la vallécule. Le traitement du kyste de la vallécule consiste en une incision cervicale. A simple aspiration is recommended to decompress the cyst in emergency situations because the recurrence rate is high
| [5] | Chen EY, Lim J, Boss EF, et al. Transoral approach for direct and complete excision of vallecular cysts in children. International Journal of Pediatric Otorhinolaryngology. 2011 Sep; 75(9): 1147-1151.
https://doi.org/10.1016/j.ijporl.2011.06.007 |
[5]
. Several authors recommend the marsupialization of the cyst by electrocoagulation or with carbon dioxide (CO2). Vallecular cysts cause supraglottic obstruction due to their mass effect. The displacement of the epiglottis backward and downward leads to airway obstruction resulting in episodes of apnea and cyanosis. Poor weight gain and insufficient development are linked to the progressive increase in the size of the cyst, which interferes with swallowing
| [6] | Singh J, Jain N, Jajoo M, Roy S, Narang E, Mahajan N. Varied Clinical Presentation and Management of Paediatric Vallecular Cyst. Sultan Qaboos Univ Med J. 2021 Nov; 21(4): 639-643.
https://doi.org/10.18295/squmj.4.2021.013 |
[6]
. Our objective was the diagnostic, therapeutic and progressive aspects.
2. Observation
This was a 6-year-old female patient, a student, residing in Kayes with no medical or surgical history, who was admitted for progressive pharyngeal discomfort that had been developing for 3 months. The onset was marked by a sensation of pharyngeal discomfort associated with a notion of serous anterior rhinorrhea, an unquantified fever, and a dry cough. This required several unsuccessful treatments. The evolution was marked by the appearance of an intraoral mass. This mass appeared a month ago.
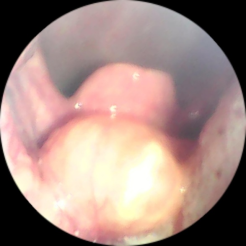
On oropharyngoscopic examination, we noted the presence of a mass which overhung the free edge of the epiglottis occupying almost the entire oropharyngeal passage
Figure 1.
Figure 1. Endoscopic view of the vallecular cyst.
At the nasofibroscopy we highlighted a soft, oval, transluminal mass, with regular contours, non-painful, non-bleeding on contact, measuring approximately 5 cm in diameter at the level of the right vallecula. The rest of the examination of the other devices was normal. We concluded that it was a vallecula cyst
Figure 2.
Figure 2. Endoscopic view after excision of the vallecular cyst.
A coordinated airway management plan was established by the anesthesiologist-surgeon before the procedure.
Excisional surgery was performed under general anesthesia with orotracheal intubation.
Patient in the supine position, headrest under the head and roller under the shoulders.
After placement of the Kilner mouth opener. Exposure and grasping of the mass. The mass was oval, soft in consistency. During surgery, accidental perforation of the mass was performed, allowing approximately 8 cc to flow. Excision of the cystic pocket was performed with the electric scalpel [
Figure 3].
In the immediate postoperative period following extubation, we did not observe any dyspnea.
The histological result of the surgical specimen concluded that there was fibrous and inflammatory squamous tissue. After six months of follow-up, we have not noted any recurrence.
3. Discussion
Abercrombie described vallecular cysts in 1881
| [6] | Singh J, Jain N, Jajoo M, Roy S, Narang E, Mahajan N. Varied Clinical Presentation and Management of Paediatric Vallecular Cyst. Sultan Qaboos Univ Med J. 2021 Nov; 21(4): 639-643.
https://doi.org/10.18295/squmj.4.2021.013 |
[6]
. Vallecular cyst is known by different names: conservation mucous cyst, epiglottic cyst, base of tongue cyst, congenital cyst and recently, canalicular cyst
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
[1]
. This cyst forms when the duct of a mucous gland or cryptic lingual tonsils is obstructed and dilated
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
[1]
. Two main theories explain the pathogenesis of vallecular cyst which is a consequence of ductal obstruction of mucous glands or embryological malformation. Histologically, the cyst contains respiratory epithelium with mucous glands and an outer lining of squamous epithelium
| [6] | Singh J, Jain N, Jajoo M, Roy S, Narang E, Mahajan N. Varied Clinical Presentation and Management of Paediatric Vallecular Cyst. Sultan Qaboos Univ Med J. 2021 Nov; 21(4): 639-643.
https://doi.org/10.18295/squmj.4.2021.013 |
| [7] | Doumbia-Singare K, Timbo SK, Diakite AA, Troare L, Guindo B, Soumaoro S, et al. Vallecular cyst: about 3 observations. Rev Col Odonto-Stomatol Afr Maxillofacial Surg 2015; 22(2): 33-36. |
[6, 7]
. The cyst can be located on the lingual surface of the epiglottis
| [8] | Parelkar SV, Patel JL, Sanghvi BV et al. An unusual presentation of vallecular cyst with near respiratory distress and management using conventional laparoscopic instruments. J Surg Tech Case Rep. 2012; 4(2): 118-20.
https://doi.org/10.4103/2006-8808.110257 |
[8]
. Chronic inflammation, leading to obstruction of the mucus glands, is thought to be the main cause
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
[1]
. However, a congenital etiopathogenesis has also been considered because some vallecula cysts have been described in newborns
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
| [9] | Puneeth PJ, Balushi F, Gandhi S. Vallecular Cyst: 10 Years Experience and Review of the Literature. Indian Journal of Otolaryngology and Head & Neck Surgery. 2023; 75: 492-95. https://doi.org/10.1007/s12070-022-03319-3 |
[1, 9]
.
Vallecular cysts resembling tonsillar crypts due to associated lymphoid tissue have been separately classified as lymphoepithelial cysts and may also occur in the aryepiglottic fold, vestibule, and piriform sinus
| [10] | Romak JJ, Olsen SM, Koch CA, Ekbom DC. Bilateral vallecular cysts as a cause of Dysphagia: case report and literature review. Int J Otolaryngol. 2010; 2010: 697583.
https://doi.org/10.1155/2010/697583 Epub 2010 Dec 12. |
[10]
. These vallecular cysts are often multiple, as reported by Romak JJ. He reported two vallecular cysts in a 70-year-old woman.
Symptoms vary according to age and size of the cyst. In children, vallecula cysts are potentially fatal, causing airway obstruction. In this case, the cyst may present with stridor and respiratory distress. The most serious complication is respiratory failure or death due to an upper airway obstruction, which is more likely to occur when the cyst is large and close to the laryngeal inlet
| [11] | Alnaimi A, Abushahin A. Vallecular Cyst: Reminder of a Rare Cause of Stridor and Failure to Thrive in Infants. Cureus. 2021 Nov 18; 13(11): e19692.
https://doi.org/10.7759/cureus.19692 |
[11]
. This is explained by the narrowness of the laryngeal passage in children. However, in adults, the symptoms are less dangerous and may manifest as dysphagia, pharyngeal paresthesias such as a foreign body sensation, or dysphonia. Vallecula cysts are asymptomatic and are discovered during a routine laryngeal examination, intubation, or radiological examination
. Vallecular cyst occurs at any age but is less common in children than in adults. Our case is similar to that of Puneeth PJ in whom the age of discovery was from birth to 8 years
| [9] | Puneeth PJ, Balushi F, Gandhi S. Vallecular Cyst: 10 Years Experience and Review of the Literature. Indian Journal of Otolaryngology and Head & Neck Surgery. 2023; 75: 492-95. https://doi.org/10.1007/s12070-022-03319-3 |
[9]
. We performed a nasofibroscopy, which was our first-line examination. Direct laryngoscopy, under general anesthesia, allows for diagnostic certainty and the elimination of laryngomalacia, which is frequently associated with vallecular cyst and is the leading cause of stridor in children
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
| [12] | Raftopulos M, Soma M, Lowinger D, et al. Vallecular cysts: a differential diagnosis to consider for neonatal stridor and failure to thrive. JR Soc Med Sh Rep. 2013; 4: 29.
https://doi.org/10.1177/2042533313476689 |
[1, 12]
.
The vallecular cyst can be detected prenatally with ultrasound and magnetic resonance imaging. It will allow for parental counseling and perinatal preparation. Precautions should be taken in cases of dyspnea due to compression on the epiglottis, which can lead to airway obstruction. After birth, the authors report that direct laryngoscopy is an effective diagnostic method; in our case, nasofibroscopy was performed. Direct laryngoscopy allowed for the excision of the cyst.
Haemangioma, cystic hygroma, teratoma, hamartoma, dermoid cyst, lymphangioma, thyroglossal duct cyst, and thyroid remnant cyst should be considered in the differential diagnosis of vallecular cyst
| [13] | Gogia S, Agarwal SK, Agarwal A. Vallecular cyst in neonates: case series-a clinicosurgical insight. Case Rep Otolaryngol. 2014; 2014: 764860.
https://doi.org/10.1155/2014/764860 Epub 2014 Oct 28. |
[13]
Postnatally, ultrasound can be used to screen for congenital stridor. It allows distinction between a cystic and a solid mass.
We did not perform postnatal imaging; the nasofibroscopy allowed us to detect the cyst.
| [8] | Parelkar SV, Patel JL, Sanghvi BV et al. An unusual presentation of vallecular cyst with near respiratory distress and management using conventional laparoscopic instruments. J Surg Tech Case Rep. 2012; 4(2): 118-20.
https://doi.org/10.4103/2006-8808.110257 |
[8]
Imaging such as CT and MRI are useful in the diagnosis of vallecular cysts, especially deep ones, not recognized by laryngeal fibroscopy. They allow the nature, location and extent of the lesion to be specified
| [9] | Puneeth PJ, Balushi F, Gandhi S. Vallecular Cyst: 10 Years Experience and Review of the Literature. Indian Journal of Otolaryngology and Head & Neck Surgery. 2023; 75: 492-95. https://doi.org/10.1007/s12070-022-03319-3 |
[9]
. Ultrasound or CT confirms the fluid nature of the lesion. The vallecular cyst appears on ultrasound as a median, anechoic, well-defined, thin-walled mass of variable size, generally large and more or less obstructive in the oropharyngeal lumen
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
| [3] | Lengane NI, Ouermi AS, Some MJ, Coulibaly A, Kadyogo M, et al. Vallecular cyst in children: a report of 3 cases. African Journal of Clinical Cases and Reviews 2020; 4(3): 287-90. |
[1, 3]
. However, CT remains the essential examination, objectifying a regular, homogeneous, hypodense supraglottic mass, which does not take up contrast except in the case of superinfection
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
| [2] | Mehdi H, Mohamed J, Nouha Ben H, Khalifa M, et al. Symptomatic vallecular cyst in adults: a report of 4 cases. Pan African Medical Journal. 2018, 31: 36.
https://doi.org/10.11604/pamj.2018.31.36.16333 |
| [4] | Hariga I, Mardassi A, Zribi S, Charfeddine A, Amor MB, Gamra OB, et al. The vallecula cyst: about 2 observations. J. TUN ORL 2008; 20: 45-48. |
[1, 2, 4]
. MRI shows a lesion of the same intensity as the CSF in T1 (hyposignal) and T2 (hypersignal). However, it does not appear to provide any information superior to that of the scanner, which should remain the first-line examination
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
| [2] | Mehdi H, Mohamed J, Nouha Ben H, Khalifa M, et al. Symptomatic vallecular cyst in adults: a report of 4 cases. Pan African Medical Journal. 2018, 31: 36.
https://doi.org/10.11604/pamj.2018.31.36.16333 |
| [4] | Hariga I, Mardassi A, Zribi S, Charfeddine A, Amor MB, Gamra OB, et al. The vallecula cyst: about 2 observations. J. TUN ORL 2008; 20: 45-48. |
[1, 2, 4]
. We did not perform imaging because the diagnosis was made by nasofibroscopy and suspension laryngoscopy.
The treatment of vallecular cyst is surgical and the endoscopic approach, using a laryngoscope, is widely used
| [12] | Raftopulos M, Soma M, Lowinger D, et al. Vallecular cysts: a differential diagnosis to consider for neonatal stridor and failure to thrive. JR Soc Med Sh Rep. 2013; 4: 29.
https://doi.org/10.1177/2042533313476689 |
[12]
. During endoscopic treatment, several procedures can be performed, including aspiration, marsupialization and excision of the cyst
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
| [4] | Hariga I, Mardassi A, Zribi S, Charfeddine A, Amor MB, Gamra OB, et al. The vallecula cyst: about 2 observations. J. TUN ORL 2008; 20: 45-48. |
| [12] | Raftopulos M, Soma M, Lowinger D, et al. Vallecular cysts: a differential diagnosis to consider for neonatal stridor and failure to thrive. JR Soc Med Sh Rep. 2013; 4: 29.
https://doi.org/10.1177/2042533313476689 |
[1, 4, 12]
. Cyst aspiration in the face of intubation difficulties and the extent of respiratory distress followed by marsupialization is widely recommended by the authors
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
| [12] | Raftopulos M, Soma M, Lowinger D, et al. Vallecular cysts: a differential diagnosis to consider for neonatal stridor and failure to thrive. JR Soc Med Sh Rep. 2013; 4: 29.
https://doi.org/10.1177/2042533313476689 |
[1, 12]
. The external cervical approach is indicated in the case of recurrent or large vallecular cyst
| [1] | Samaké D, Sidibé Y, Koné FI, Diarra A, Bagayoko DK, Kanté M, et al. Vallecular cyst complicated by severe acute malnutrition in children: clinical and therapeutic characteristics. J. TUN ORL 2023; 33(50): 30-33. |
[1]
. This technique is aggressive with a risk of pharyngostoma and cervical scar
| [3] | Lengane NI, Ouermi AS, Some MJ, Coulibaly A, Kadyogo M, et al. Vallecular cyst in children: a report of 3 cases. African Journal of Clinical Cases and Reviews 2020; 4(3): 287-90. |
| [12] | Raftopulos M, Soma M, Lowinger D, et al. Vallecular cysts: a differential diagnosis to consider for neonatal stridor and failure to thrive. JR Soc Med Sh Rep. 2013; 4: 29.
https://doi.org/10.1177/2042533313476689 |
[3, 12]
.
In our case, the intraoral route was performed, using a KILNER mouth opener, excision surgery with aspiration of the cyst contents was performed under general anesthesia with orotracheal intubation.
This therapeutic attitude is recommended by several authors
| [4] | Hariga I, Mardassi A, Zribi S, Charfeddine A, Amor MB, Gamra OB, et al. The vallecula cyst: about 2 observations. J. TUN ORL 2008; 20: 45-48. |
| [12] | Raftopulos M, Soma M, Lowinger D, et al. Vallecular cysts: a differential diagnosis to consider for neonatal stridor and failure to thrive. JR Soc Med Sh Rep. 2013; 4: 29.
https://doi.org/10.1177/2042533313476689 |
[4, 12]
.
The normal appearance of the cyst covering mucosa and the close adherence of the cyst lining to the muscular fibers of the tongue, with no preexisting dissection plane, were also noticed during surgery as in the case of Zamfir-Chiru-Anton A
| [14] | Zamfir-Chiru-Anton A, Gheorghe DC. Vallecular cysts in clinical practice: report of two cases. J Med Life. 2016 Jul-Sep; 9(3): 288-290. |
[14]
During surgery, an accidental rupture of the cyst occurred, releasing approximately 8 cc. We performed a complete excision of the cystic pocket using an electric scalpel.
We have not noted any recurrences the negligible recurrence rate after marsupialization has been reported in the literature
| [15] | Jason M. Leibowitzb, Lee P. Smitha, Marc A. Cohenb, Brian P. Dunhama, b, Marta Guttenbergc, Lisa M. Elden. Diagnosis and treatment of pediatric vallecular cysts and pseudocysts. International Journal of Pediatric Otorhinolaryngology 2011; 75: 899–904. https://doi.org/10.1016/j.ijporl.2011.03.032 |
[15]
.
Author Contributions
Toure Tata: Conceptualization
Ouane Aissata: Conceptualization, Investigation, Methodology, Writing – review & editing
Coulibaly Assitan Kole: Conceptualization, Investigation, Methodology, Writing – review & editing
Dicko Ibrahim: Formal Analysis, Writing – original draft
Diamoutene Boubacar Sidiki: Formal Analysis
Diakite Zoumana: Formal Analysis
Famagan Bah: Software, Writing – original draft
Doumbia Salim: Writing – original draft
Cisse Naouma: Project administration, Writing – review & editing
Konate N’faly: Project administration
Diarra Kassim: Project administration
Kone Fatogoma Issa: Investigation, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing
Guindo Boubacary: Resources, Software
Soumaoro Siaka: Conceptualization, Data curation, Investigation, Methodology, Visualization
Singare Kadidiatou: Software
Keita Mohamed Amadou: Software, Validation